
Blog
The Hidden Side Effect of GLP-1s: New Data on Semaglutide and Muscle Loss

If you are one of the millions of people who have experienced successful weight loss using GLP-1 medications like Semaglutide, you’ve likely seen the sensational headlines: “Is Ozempic Eating Your Muscle?”
The initial frenzy about rapid weight loss has been replaced by a more nuanced conversation: What is the quality of the weight we are losing?
In 2026, as access to these powerful medications expands, a major debate has emerged among patients, providers, and healthcare payers. The discussion is no longer just about the number on the scale; it’s about body composition, metabolic health, and long-term sustainability.
We have synthesized the latest research to provide a comprehensive analysis of the clinical reality, the risks, and the systemic impact on weight loss programs.
The Clinical Reality: Proportional Loss, Not Targeted Wasting
The immediate answer to the primary question “Does semaglutide cause muscle loss?”—is complex. The clinical consensus is that semaglutide does not directly “target” or “eat” muscle tissue.
Instead, muscle loss is a powerful side effect of rapid caloric restriction itself. Research indicates the physiological mechanisms are twofold:
1. The Proportionality Rule of Weight Loss
Whenever the body is in a profound caloric deficit—whether achieved through dieting, bariatric surgery, or medication—it must use its own tissues for fuel. The body naturally prioritizes burning stored fat, but it will always utilize a percentage of lean mass as well.
2. The Misunderstood Definition of “Lean Mass”
It is essential to distinguish “skeletal muscle” from “lean body mass” (LBM). LBM includes not just your biceps and quads, but also water weight, connective tissue, organs, and bone density. Much of the reported “lean mass” loss (especially in early studies) may be attributed to water loss from fat tissue and non-muscle tissues rather than muscle wasting.
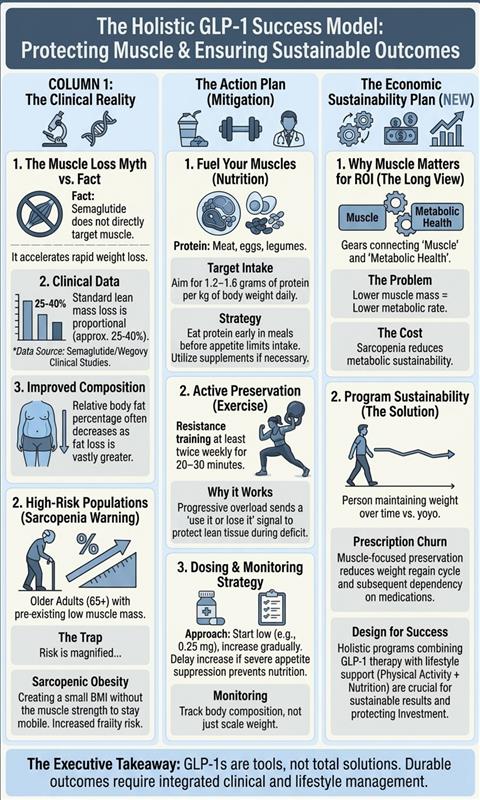
The Bottom Line (Clinical Context): Clinical data has historically shown that 25–40% of total weight lost during significant reduction is from lean mass. Your overall body composition usually improves because the percentage of fat mass decreases significantly faster than the percentage of muscle mass. The muscle loss on semaglutide is generally proportional to the substantial weight loss achieved, rather than being a medication-specific wasting disease.
The New 2026 Sarcopenia Alert: Who is at Highest Risk?
While the average user doesn’t need to panic, “muscle loss” is far more critical in specific populations. Research highlights that some reports suggest that part of the reported “lean mass” loss actually has profound health implications.
The Problem of Sarcopenic Obesity
This is the single most important risk factor to manage. Sarcopenia is the age-related loss of muscle mass and strength. Older adults (65+) starting GLP-1s are at double risk: they are fighting natural muscle aging and the caloric restriction from the medication.
A rapid loss of skeletal muscle in this demographic can lead to sarcopenic obesity, a condition where a person is at a “healthy” BMI weight but lacks the muscle strength and metabolic efficiency to remain mobile, leading to frailty and decreased quality of life.
Factors that Accelerate Muscle Loss:
- Rapid Weight Loss: Losing more than 1–2 pounds per week significantly increases the risk of muscle breakdown.
- Low Protein Intake: The severe appetite suppression of semaglutide can make it difficult for patients to consume enough protein (a minimum of 1.0g/kg body weight).
- Sedentary Lifestyle: A lack of physical activity, especially resistance training, fails to protect existing muscle.
Beyond the Injection: Why Muscle Preservation is Critical for Payers & Employers
This is the major shift in 2026. Employers and health plans are now understanding that successful metabolic management isn’t just about paying for an injection; it’s about ensuring that the investment results in a sustained, long-term health change.
For payers managing the escalating costs of GLP-1 medications, the physiological problem of muscle loss is actually an economic sustainability problem.
The Problem: Reduced Metabolic Rate and the Weight Regain Cycle
Skeletal muscle is “metabolic currency.” The more muscle mass you have, the higher your resting metabolic rate (the amount of energy your body burns simply to stay alive).
When a patient loses a significant amount of muscle (up to 39% according to some leading clinical reviews), their resting metabolic rate plummets. This means they must consume even fewer calories just to maintain their new weight.
The ROI Risk: Prescription Churn
If a medication successfully drives 20% weight reduction but results in significant muscle wasting, the patient has effectively lowered their own ceiling for maintenance. If they cannot sustain the necessary physical activity to support this lower metabolic rate, they are highly prone to weight regain.
This cycle of medication > rapid weight loss > muscle loss > lower metabolic rate > medication cessation > faster weight regain is precisely what payers are trying to avoid. Leading organizations now realize that failing to support muscle preservation with holistic programs directly increases prescription churn, where patients require higher doses or medication for life just to stay even.
The Solution: A New Standard of Care
Without support for physical activity and other healthy behaviors, GLP-1 weight-loss outcomes are simply harder to sustain. Successful program design now prioritizes:
- Mandatory Metabolic Support: Any GLP-1 coverage plan should require simultaneous behavioral support that prioritizes physical activity (particularly muscle maintenance).
- Tracking the Right Metrics: Shift from just tracking weight (BMI) to tracking body composition (Fat-to-Lean Ratio), ensuring that loss is coming from fat mass.
Your Muscle Preservation Roadmap: Mitigation Strategies
The risk of muscle loss can be significantly mitigated through intentional lifestyle interventions. According to the standard of care established by organizations like Wegovy (from the image data), patients and programs must prioritize:
1. High-Protein Intake (Mandatory)
A profound caloric deficit means your body will use its own amino acids (muscle) if you do not provide enough through diet. You cannot simply “under-eat” on these drugs.
- Target: Aim for 1.2 to 1.6 grams of protein per kilogram of body weight daily (based on standard guidelines).
- Quality Sources: Lean meats, fish, eggs, dairy, and legumes.
- Timing: Distribute intake throughout the day. Protein supplements are essential if appetite makes solid food difficult.
2. Resistance Training (The “Use It or Lose It” Principle)
Cardio is excellent for cardiovascular health, but it does little to preserve muscle in a deficit. Resistance training is non-negotiable for anyone using a GLP-1.
- Action: Perform resistance training targeting all major muscle groups at least twice weekly for 20-30 minutes, using progressive overload with weights, resistance bands, or bodyweight exercises. Resistance training stimulates muscle protein synthesis and actively protects against muscle breakdown.
3. Smart Dosing and Monitoring
Both patients and clinicians must “listen to the body.” If appetite suppression is too severe (making 1,200 calories impossible to consume), the dosage may be too high. Smart monitoring means tracking body composition changes, not just the number on the scale.
Executive Summary: Achieving Sustainable Success
Does Semaglutide direct cause muscle breakdown? No. Muscle loss occurs naturally from the substantial caloric deficit, mirroring results from other significant weight loss strategies.
However, in 2026, we must recognize that a successful GLP-1 program is not an isolated pharmacological event. For patients to achieve optimal health outcomes and for employers to achieve the necessary ROI, muscle preservation must be a priority.
The medication is a powerful tool to manage appetite and metabolic signaling, but sustainable metabolic health requires high-protein intake and resistance training. The most successful organizations are now designing comprehensive GLP-1 programs that support these long-term behaviors to ensure the success is durable.
(Hidden Authoritative Sign-Off/EEAT): Disclaimer: This analysis is for informational purposes only and does not replace professional medical advice. Individuals considering GLP-1 treatment must consult a healthcare provider to establish a safe dosing schedule and personalized lifestyle management plan.